The purpose of this page is to share information about the importance of nutritional lithium in human biology, not to be confused with prescription/pharmaceutical lithium at 100-300 times higher doses.
Per the update log, this page was last updated in 2017. Moreover, since migrating to a new host in ~2021, .not all images are hosted properly yet!
Table of Contents
- 1. “I thought lithium was for crazy people!“
- 2. Lithium, chemistry, and common sense
- 3. Lithium and Longevity
- 4. Lithium and Pregnancy
- 5. Lithium and Suicide
- 6. What should/can I do?
- Appendix A: Units of measurement
- References
- Lithium and Headaches/Obesity [anecdotal]
- Hypotheses and Ideas Regarding Lithium (obesity, cravings, postpartum depression, food/water levels, insomnia, etc.)
- Special Thanks
- Comments & Feedback
- [Update Log]
1. “I thought lithium was for crazy people!”
At high dosages, lithium is used as a very effective drug for clinical patients. However…
Lithium is an essential dietary nutrient whose provisional RDA was proposed in 2002 at 1mg/day for the average adult 1 .
It is critical that lithium as an essential nutrient not be confused with prescription lithium. There, it is prescribed at doses of 100-300+ mg/day. Nutritional (left) and prescription levels (right) compared visually:
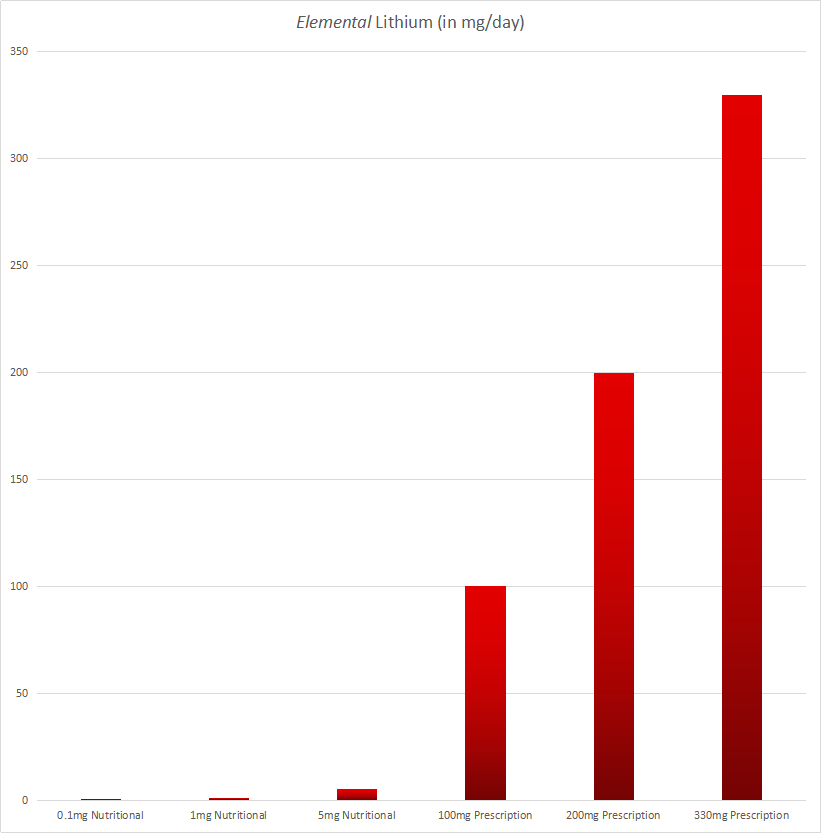
*Neither 0.1mg nor 5.0mg/day are recommended intakes. The former may result in deficiency, depressive symptoms and worse, and the latter may be excessive in the long term and may cause a minor /headache. These numbers are simply shown to visually illustrate the order-of-magnitude differences between referring to “nutritional” lithium and “pharmacological/therapeutic/prescription” lithium.
Comparing the two would be similar to comparing the vitamin B-6 consumed from eating a spinach salad with the B-6 consumed from chugging ten energy drinks!
B-6 in ~300g spinach : 30%
B-6 in 10 energy drinks : 20,000%
For a few good non-scientific web articles, see these external links:
- A 2012 blog post from the magazine Psychology today, “Could You Have a Lithium Deficiency? Shocking but true. Lithium is an essential trace element.“, or
- a New York Times opinion from 2014, “Should We All Take a Bit of Lithium?“
2. Lithium, chemistry, and common sense
A) THE PERIODIC TABLE IS BEAUTIFUL:

Images credit: www.ptable.com
If you think the periodic table is boring, you’re probably stuck with that thinking from chemistry class in high school. And I agree, it was boring.
However, if you learn a little about chemistry as an adult, and you have a good teacher (try Khan Academy!), you’ll likely agree with most scientists on at least one point: the periodic table is one of the most beautiful groupings of information ever created by humans.
It may not be an expensive piece of artwork, but it’s gorgeous: every number, position, row, column, and other piece of information has meaning. Physics’ “the standard model” might be a close second, but it’s still very modern, contested, and not very useful in our daily lives. I’m partial to biology because of my background, but let’s admit it: the biological model of “the cell” is far too young, and can’t account for a) everything we don’t know, or b) everything that exists outside that cute little textbook cell illustration (viruses, nutrients, etc.). “Higher” sciences, like economics or psychology, are decades away from even beginning to classify their information onto a single powerful page like this one.
Say it with me: chemistry’s periodic table of the elements is beautiful!
B) BASICS
Let’s review some basics as they’re applicable to biology:
- Each numbered square is an element — or atom. In biology, they don’t often exist alone, they’re bound to other groups of atoms forming a molecule.
- Elements in the same column (above and below each other) have similar outer electron shells, which means they tend to behave similarly. Think of (and look at) these three for a good example: copper (29), silver (47), and gold (79).
- More “reactive” elements are to the far left and far right of the table, with the exception of column 18: the noble gasses. The noble gasses don’t react chemically and are “stable,” but rows 1 and 17 are extremely reactive elements, and each column on towards the middle is less so.
- Like many elements, lithium doesn’t exist in nature in its reactive, elemental form. It’s almost always bound to a molecule, which is why it’s taken (nutritionally or pharmaceutically) through forms like lithium -chloride, -carbonate, -aspartate, -orotate, etc. But its’ position on the periodic table should indicate how reactive it is.
- Each additional row from the top down has an additional “shell” or layer of electrons, making the atoms/elements in that row more “complex,” in a sense.
C) LOGIC AND COMMON SENSE
The “highest” element known to be used in the human body is iodine (53). Let’s start with a greyscale periodic table, ignoring everything past iodine:

Now let’s highlight the more “conventional” elements accepted to be used as nutrients within the human body. You can still find images like this online, without lithium noted:

Now, here’s the chart with lithium:

It’s possible other higher elements are used as well, like nickel or bromine. We won’t be sure for many, many years.
But asserting, for instance, that an element like tellurium (52, under selenium) plays a biological role in the human body is an extraordinary claim requiring extraordinary evidence.
Lithium, on the other hand, doesn’t require such an assertion. Lithium’s place on a “biological periodic table of elements” is neither controversial nor unknown. It’s simply been ignored. More importantly, considering its chemical position between hydrogen, sodium, and potassium, it also “makes sense” from a logical perspective.
3. Lithium and Longevity
A) Lithium and other biological species
At high dosages, lithium has increased survival, longevity, and progeny (children) in the worm C. elegans 21, 22 , and in the fly Drosophila melanogaster 23. Both are biological “model” organisms used to study biological effects before (or concurrently) looking at effects in humans.
B) Lithium and Human Longevity
Within science, phrases like “all cause mortality” or “mortality” refer to every possible cause for human death. Anything significant enough to reduce all overall causes of mortality — like exercise and fasting — is bound to be investigated more and more as research money becomes available.
In 2011, European researchers concluded “that long-term low-dose exposure to lithium may exert anti- aging capabilities and unambiguously decreases mortality in evolutionary distinct species” 16 [emphasis added].
Unfortunately, as lithium is not yet a recognized nutrient by the FDA/WHO, little research money is available to study it.
4. Lithium and Pregnancy
A) Nutritional levels
In the 2002 paper 1 which recommended a provisional RDA for lithium, the author, an expert trace mineral researcher, made several comments regarding lithium and pregnancy. All emphasis below (bolding and italics) is added:
- “Lithium appears to play an especially important role during the early fetal development as evidenced by the high lithium contents of the embryo during the early gestational period.”
- “During embryonic development, organ lithium levels reach maximal values in the first trimester of gestation and subsequently decline, as is true for other trace elements.”
- “The fact that embryonal Li concentrations are the highest during early fetal development suggests that it is specifically needed.”
- “…the possibility that inadequate Li intakes cause behavioral defects should be considered.”
- “Special attention should be accorded to the potentially higher relative Li needs of children, adolescents and lactating mothers.“
- “An adequate supply of Li should also be assured for subjects on formula diets and or on total or home parenteral nutrition.”
- 1 [all emphasis added]
Due to connections with vitamins B-9 and B-12 metabolism, lithium is likely as important as nutritional folate supplementation and should be recommended appropriately.
In 2006, researchers noted that low levels of lithium were even associated with autism. They concluded “Low lithium in the mothers likely caused low levels of lithium in the young children, which could have affected their neurological and immunological development” and recommended further investigations of these elements ” 15 [emphasis added].
B) Wait… isn’t lithium teratogenic?
Teratogenic: a molecule which can disturb a developing embryo or fetus.
In other words, a “teratogenic” substance/drug/food/etc. is dangerous to a developing baby.
Examine.com does not yet cover lithium, though as a customer of their paid product, I am urging them to do so. I believe they are potentially hurting pregnant mothers when they write, on the page “What supplement or food changes are recommended for pregnant or expecting women?“, that both
- only three substances: folate, choline, and ginger are generally safe for pregnant mothers, and
- and that “lithium, at certain [high] dosages” might be a teratogen (dangerous).
This is dangerous, as it may steer pregnant mothers away from the use of nutritional lithium, when in practice, lithium might even be more important than folate (B-9).
Examine.com only notes two studies looking into whether lithium might be teratogenic or not. Both studies look at lithium as a prescription/theraputic drug, and are not relevant to lithium as a nutrient. Still, so expecting parent’s might feel more comfortable, I will link to them anyway:
- Giles JJ, Bannigan JG. Teratogenic and developmental effects of lithium. Curr Pharm Des. (2006)
- Yacobi S, Ornoy A Is lithium a real teratogen? What can we conclude from the prospective versus retrospective studies? A review. Isr J Psychiatry Relat Sci. (2008)
There are more results when one searches the scientific literature for both “lithium” and “teratogenic,” among other combinations. However, nearly all studies refer to lithium as a prescription drug. Studies investigating lithium as a potential teratogen (like those two above) look at prescription lithium, at dosages of 100-300+mg/day, on patients being prescribed this lithium (usually lithium chloride or carbonate) by their doctors. Again, there is no comparison to low-levels of lithium consumed through food and responsible supplementation. And even both studies above do not show convincing evidence that high-dose, prescription lithium is a teratogen.
For that reason, the authors of the first study above note that “[therapeutic] lithium is a “weak” teratogen in humans,” and the authors of the second study above say “lithium [as a drug] does not seem to be a significant teratogen, and hence should be given, if indicated [by a medical doctor], in pregnancy.”
Please remember:
At reasonable dosages, there is no evidence of a nutrient that is dangerous to the developing fetus. For concerned/expecting parents, I’ll write that sentence again:
At reasonable dosages, there is no evidence of a nutrient that is dangerous to the developing fetus. Please /contact me immediately if I am incorrect (for instance, if that statement isn’t true for an element like vanadium or molybdenum.)
As usual, you must dissociate a doctor’s usage of the word “lithium” and his/her mental picture of “lithium chloride at 300-2,000+mg/day” from the usage of the term “nutritional lithium” with the 0-3mg elemental lithium a human might consume during a typical day.
Consuming 0mg of lithium per day through diet alone might be extremely dangerous to a developing embryo/fetus, and we have no knowledge of typical nutritional lithium dosages in most foods and water supplies. From a scientific perspective, low-dosage nutritional lithium supplementation is extremely safe for pregnant women. See the hypotheses section below for more.
The benefits (massive) far outweigh the risks (nonexistent at nutritional dosages).
C) Conclusion
I do not recommend you ask your doctor for permission to supplement responsibly with low levels of this nutrient.
I recommend you make an informed decision and then converse with or tell your doctor about your decision. Feel free to print this page. You must remind your doctor that his/her knowledge came from a medical school and society which only views the word “lithium” as a high-dosage prescription drug and not the essential nutrient that it is at low levels.
Government funding works incredibly slowly. Science works even slower. And medicine? Medicine is always decades behind both the early evidence and the money to research it.
5. Nutritional lithium and suicide
Nutritional lithium in our water supplies and suicide
Positive associations:
The association between lithium in the water supply and suicide has been discussed in multiple studies:
- In Lithuania in 2017, which “suggested that higher levels of lithium in public drinking water are associated with lower suicide rates in men” 19 ,
- 2017 in Chile, which noted “Chilean regions rich in naturally occurring lithium salts show lower suicide mortality rates in comparison to other regions” and that such studies “warrant further research on the effects of naturally occurring low-dose lithium on health” 20 ,
- 2013 in Texas, which gave “confirmatory evidence that higher lithium levels in the public drinking water supply are associated with lower suicide rates” 3 ,
- Japan in 2013, stating, conservatively, that “natural levels of lithium in drinking water might have a protective effect on the risk of suicide among females” 11,
- Greece in 2013, noting “lower suicide rates in the prefectures with high levels of lithium in drinking water” 9,
- Austria in 2011, concluding “that geographic regions with higher natural lithium concentrations in drinking water are associated with lower suicide mortality rates” 4,
- Japan in 2011, noting in addition to selenium’s importance, that “Li deficiency as well as suboptimal vitamin B12 status must be considered as potential suicide risk factors” 17,
- Japan in 2009, concluding “that even very low levels of lithium in drinking water may play a role in reducing suicide risk within the general population” 5,
- Texas in 1990, noting that “rates of suicide, homicide, and rape are significantly higher in counties whose drinking water supplies contain little or no lithium than in counties with [some] water lithium levels,” and even suggesting “that lithium at low dosage levels has a generally beneficial effect on human behavior” 6, emphasis added, and
- Texas in 1970, noting that higher “lithium content in residential drinking water” was associated with lower “diagnoses of personality disorder, psychosis, and neurosis” in hospital admission data 7. (This study did not specifically note suicide, but is the earliest related reference I’ve seen).
Negative associations:
I’m aware of two no-results (no association between lithium water levels and suicide) :
- In 2017, an analysis in the Danish population noted “no protective effect” of lithium on suicide. This could potentially be because, among other factors, Danish diets already include sufficient lithium. 18.
- England in 2011, noting “no association between lithium in drinking water and suicide rates across the East of England from 2006 to 2008″ 10.
In science, a few negative results with a vast body of positive results indicate the research creeping towards causation.
In other words, low lithium levels clearly seem to be one contributing factor to suicide.
Prescription lithium and suicide
- A 2013 meta-analysis of 48 studies concluded that “Lithium is an effective treatment for reducing the risk of suicide in people with mood disorders,” further noting “evidence that lithium decreases aggression and possibly impulsivity” 12 [emphasis added].
- In a 2006 meta-analysis, prescription lithium reduced attempted and completed suicides by about 80% (or five-fold) 2.
- In 2003, a meta-analysis of 34 studies of unipolar and bipolar patients noted a 93% reduction in suicidal acts 12! Also in 2003, a
- In 2001, a meta-analysis showed that suicide was 82% less frequent during lithium treatment 7.
These findings from prescription and nutritional lithium show that it is reasonable to conclude that nutritional lithium at lower dosages over longer periods of time almost certainly reduces suicides.
Why don’t we understand suicide better?
That’s a very complicated topic, but here’s a good response, written in 2009: “Suicide is a complex behavior, complicated to study in humans, and impossible to fully reproduce in animal models.” 14 [emphasis added].
3. What can/should I do?
First, we need to correct our own deficiencies.
See the /pills page for how I supplement (a $9 bottle of lithium orotate, Amazon.com link here). 1mg/day is the provisional RDA and it’s what I recommend, although nutritional intakes of up to 10mg/day have been reported in the scientific literature (mostly from certain South American populations with high levels of lithium in their water supplies). 2-5mg/day seems to be conservative, and I’ve experimented with this range. However, I do not recommend sustained periods of 5mg/day or more.
Remember that on most weeks, you are already consuming some lithium in your regular diet.
The question is, are you consuming enough?
I wasn’t.
Second, share this page.
There are sharing links at the top of this page and/or on the sidebar to the left. Since governments tend to do what they do best (nothing), sharing this information with others is the only way anything will improve.
Third, If you’re an American, contact the FDA (and sign the white house petition).
In general, the government doesn’t actually do anything useful unless there are large numbers of people forcing the work to be done. Lithium’s RDA was submitted in 2002, but, so shortly after the 9/11 attacks, the paper was ignored. Fifteen years later, we are paying dire consequences with our individual and societal health.
If you aren’t comfortable calling, the Food and Cosmetics Information Center (FCIC) has an “inquiry form” here which you can fill out. I recommend you click “No” in response to the FSMA question, then click on both “Food” and “Nutrition Information” in the two drop down lists.
You are welcome to copy and paste a comment such as this:
Based on the information and references from www.johnfial.com/lithium/ , the scientific evidence shows that the FDA should include lithium as a recommended mineral at 1mg/day for adult Americans.
After a text submission of my own (longer) comment, the FDA quickly responded with:
Good morning, thank you for your message. We appreciate your interest in supporting adequate nutrient intake. As you know, at this time FDA does not identify lithium as an essential nutrient. However, we are aware of emerging research on the role of lithium as a nutrient and will continue to monitor such research. If significant scientific agreement arises recommending a daily value for lithium intake, FDA may consider amending its regulations accordingly. We encourage you to support publication of peer-reviewed research into this subject. [emphasis added]
In the time between submission of my comment and receiving the above response, there were 0 new visitors to this page, which means no one from the FDA even bothered to read this. The administration will likely ignore future comments from the public, but I still encourage you to try.
Click here to contact the FDA.
Since 113 Americans will commit suicide tomorrow (see afsp here or cdc here), and since lithium is a nutrient found in food, I also recommend calling the numbers 1-866-300-4374 or 1-301-796-8240 “for an emergency regarding food.”
Appendix A: Units of measurement
Skip this section if you’re familiar with the below units.
- A penny is about 1.5 grams.
- The “milli” prefix means “one thousandth.”
- Thus, 1,000 milligrams equals 1 gram (g).
- So that 1.5g penny is about 1,500 milligrams.
- That’s about the amount of lithium carbonate clinical patients are often prescribed daily. Because you have to think about the weight of the carbonate molecule, 1,600mg lithium carbonate equates to about 300mg of pure elemental lithium. That’s a lot of lithium: nearly 300 days’ worth of the provisional RDA.
- There are 1,000 micrograms (abbreviated mcg) in 1 milligram (mg).
- 1 milligram (1mg) is lithium’s provisional RDA for the average adult.
- So that 1.5g penny is about 1,500,000 micrograms (mcg).
- A child might only need 500 micrograms or less (500 mcg, aka 0.5 mg) of lithium. Larger adults can probably safely self-experiment with a few milligrams per day.
For consistency, I’ll aim to keep this page in milligrams (mg).
References
- Schrauzer, G.N. (2002). Lithium: occurrence, dietary intakes, nutritional essentiality. Journal of the American College of Nutrition, 21(1), 14-21. ||| [Click here to read/download the original 2002 Schrauzer RDA paper. It is only 6 pages, and although it is a scientific publication, it is not overly technical and should be accessible to many readers with non-scientific backgrounds.]
- Baldessarini, R. J., Tondo, L., Davis, P., Pompili, M., Goodwin, F. K., & Hennen, J. (2006). Decreased risk of suicides and attempts during long-term lithium treatment: a meta-analytic review. Bipolar Disorders, 8(5 Pt 2), 625-39.
- Blüml, V., Regier, M. D., Hlavin, G., Rockett, I. R., König, F., Vyssoki, B., & … Kapusta, N. D. (2013). Lithium in the public water supply and suicide mortality in Texas. Journal of Psychiatric Research, 47(3), 407-411.
- Kapusta, N. D., Mossaheb, N., Etzersdorfer, E., Hlavin, G., Thau, K., Willeit, M., & … Leithner-Dziubas, K. (2011). Lithium in drinking water and suicide mortality. British Journal of Psychiatry, 198(5), 346-350.
- Ohgami, H., Terao, T., Shiotsuki, I., Ishii, N., & Iwata, N. (2009). Lithium levels in drinking water and risk of suicide. British Journal of Psychiatry, 194(5), 464-5.
- Schrauzer, G.N. & Shrestha, K.P. (1990). Lithium in drinking water and the incidences of crimes, suicides, and arrests related to drug addictions. Biological Trace Elements Research, 25(2), 105-13.
- Tondo, L., Hennen, J., & Baldessarini, R. J. (2001). Lower suicide risk with long-term lithium treatment in major affective illness: A meta-analysis. Acta Psychiatrica Scandinavica, 104(3), 163-172.
- Dawson, E. B., Moore, T. D., & McGanity, W. J. (1970). The mathematical relationship of drinking water lithium and rainfall to mental hospital admission. Diseases of the Nervous System, 31(12), 811-820.
- Giotakos, O., Nisianakis, P., Tsouvelas, G., & Giakalou, V.V. (2013). Lithium in the public water supply and suicide mortality in Greece. Biological Trace Elements Research, 156(1-3), 376-9.
- Kabacs, N., Memon, A., Obinwa, T., Stochl, J., & Perez, J. (2011). Lithium in drinking water and suicide rates across the East of England. British Journal of Psychiatry, 198(5), 406-7.
- Sugawara, N., Yasui-Furukori, N., Ishii, N., Iwata, N., & Terao, T. (2013). Lithium in tap water and suicide mortality in Japan. International Journal of Environmental Research and Public Health, 10(11), 6044-6048.
- Cipriani, A., Hawton, K., Stockton, S., & Geddes, J. R. (2013). Lithium in the prevention of suicide in mood disorders: Updated systematic review and meta-analysis. BMJ: British Medical Journal, 346, 1-13.
- Guzzetta, F., Tondo, L., Centorrino, F., & Baldessarini, R. J. (2007). Lithium treatment reduces suicide risk in recurrent major depressive disorder. Journal of Clinical Psychiatry, 68(3), 380-383.
- Kovacsics, C. E., Gottesman, I. I., & Gould, T. D. (2009). Lithium’s antisuicidal efficacy: elucidation of neurobiological targets using endophenotype strategies. Annual Review of Pharmacology and Toxicology, 49, 175-198.
- Adams, J.B., Holloway, C.E., George, F., & Quig, D. (2006). Analyses of toxic metals and essential minerals in the hair of Arizona children with autism and associated conditions, and their mothers. Biological Trace Element Research, 110(3), 193-209.
- Zarse, K., Terao, T., Tian, J., Iwata, N., Ishii, N., & Ristow, M. (2011). Low-dose lithium uptake promotes longevity in humans and metazoans. European Journal of Nutrition, 50(5), 387–389. https://doi.org/10.1007/s00394-011-0171-x
- Schöpfer, J., & Schrauzer, G. N. (2011). Lithium and other elements in scalp hair of residents of Tokyo Prefecture as investigational predictors of suicide risk. Biological Trace Element Research, 144(1-3), 418-425.
- Knudsen, N., Schullehner, J., Hansen, B., Jørgensen, L., et al. (2017). Lithium in Drinking Water and Incidence of Suicide: A Nationwide Individual-Level Cohort Study with 22 Years of Follow-Up. International Journal of Environmental Research and Public Health. 14(6), doi: 10.3390/ijerph14060627.
- Liaugaudaite, V., Mickuviene, N., Raskauskiene, N., Naginiene, R., Sher, L. (2017). Lithium levels in the public drinking water supply and risk of suicide: A pilot study. Journal of trace elements in medicine and biology, pii, doi: 10.1016/j.jtemb.2017.03.009.
- König, D., Baumgartner, J., Blüml, V., Heerlein, A., Téllez, C., Baus, N., Kapusta, ND. (2017). [Impact of natural lithium ressources on suicide mortality in Chile 2000-2009: a geographical analysis]. [Article in German]. Neuropsychiatry, 2: 70-76. DOI: 10.1007/s40211-017-0222-5
- McColl, G., Killilea, D.W., Hubbard, A.E., Vantipalli, M.C., Melov, S., Lithgow, G.J. (2008). Pharmacogenetic analysis of lithium-induced delayed aging in Caenorhabditis elegans. J Biol Chem. 283 (1) : 350-7.
- Tam ZY1, Gruber J2, Ng LF3, Halliwell B3, Gunawan R4. (2014). Effects of lithium on age-related decline in mitochondrial turnover and function in Caenorhabditis elegans. J Gerontol A Biol Sci Med Sci. 69(7):810-20. doi: 10.1093/gerona/glt210. Epub 2014 Jan 7.
- Castillo-Quan, J.I., Li, L., Kinghorn, K.J., Ivanov, D.K., Tain, L.S., et al. (2016). Lithium Promotes Longevity through GSK3/NRF2-Dependent Hormesis. Cell Rep. 15 (3):638-50. doi: 10.1016/j.celrep.2016.03.041.
Lithium and Headaches/Obesity
This is both anecdotal and hypothetical, so it’s on a separate page from the hypotheses below: /headaches.
To read about the nutrient theory of obesity, which makes even more sense in light of the lack of lithium in our food supply, see /obesity.
Other hypotheses regarding lithium
I aim to keep this “Nutritional Lithium in Human Biology” page updated with only known, scientifically supported findings. As such, the following ideas and hypotheses can be found on the /hypotheses page:
-
-
- Lithium and food cravings
- Lithium and postpartum depression
- Lithium levels in food
- Lithium in rain and ocean water
- Lithium and teenage depression/aggression
- Human hairs as trace mineral storage for the lymphatic system
-
Special Thanks To:
- Tim Ferriss and Dr. Peter Attia, whose interview in Tools of Titans introduced me to lithium as a nutrient.
- Dr. James Greenblatt and Kayla Grossmann, authors of Nutritional Lithium: A Cinderella Story, which provided me exactly what I wanted to start this page, but couldn’t find in a good review article or on the web: an expert-curated list of scientific references. (Their references are not the only place I’ve drawn from for this webpage, but they were an excellent starting point.)
Comments & Feedback
Comments on individual pages are disabled for several reasons. However, I’d love your feedback regarding this page. Please use the /contact page. Thank you!
Update Log:
[27 Jun: Minor updates to Longevity section. Note: first draft presentation video uploaded to /slides/ page.]
[1 Jun: Cleaned up chemistry section, moved to section #2.]
[30 May: added national security comment in first paragraph, moved “actions” section to #2; minor edits, added /headaches]
[25 May: Reorganized major sections, added “What should I do?” section; added the suicide section and early references, added pregnancy section and references. Also updated the first section and graph to reflect all numbers in terms of the elemental weight of lithium within the compound described. (Previously I had been comparing elemental lithium orotate with total lithium carbonate, which isn’t a fair comparison. These numbers are now a fair comparison.)]
[4 April: Reorganized; finished first decent draft of periodic table section; began “depression, anger, suicide” section.]
[22 March: Moved hypothetical sections to /hypotheses, added first graphic, revised introductory section]
[12 February 2017: created]